
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prostate Cancer
Prevention
There's no sure way to prevent prostate cancer. But you can cut your risks in half, in some cases up to 75%. Cutting risks may also reduce the tumor's growth if one does occur. See Risks.
Perhaps more importantly, you can assure against dying from prostate cancer. We explain in the next section, Risks.
Risks
Risks increase with age. This cancer strikes one in five men older than age 60. There are two ways to reduce risks. One is to avoid carcinogens --substances that spark malignant growth. Let a carcinogen turn just ONE prostate cell from healthy to malignant, and bingo! Your cancer has begun.
What's a carcinogen? A big one is flame-broiled fat in red meat, and other animal fats. Avoid - or at least minimize - fat carcinogens.
Fats that may increase prostate cancer risks are also found in butter, cream and ice cream.
Sloan-Kettering Cancer Center recommends adding the following to your daily diet as a way to reduce prostate cancer risks:
Genistein via soy 40 grams
800 IU, Vitamin E, 1000mg Vitamins A and D.
200 micrograms of selenium.
Clinical trials have shown that the proper balance and ingestion of lycopene, vitamin E, selenium, and anti-oxidants can inhibit prostate-cancer. A product called Malegard lists such preventive substances on its label.
To get the complete story on reducing prostate cancer risks, send for our Free Special Report on Diet and Prostate Cancer, also Reducing Risks of Prostate Cancer. Click here to go to the Response Form.
Finding Prostate Cancer
There is one and only one way to diagnose prostate cancer: an examination of prostate tissue under a microscope. Tissue is obtained in one of two ways. (1) A result of a trans-urethral resection of the prostate (a TURP, or "roto-rooter" surgery). (2) From a biopsy.
In most biopsies, the physician "shoots" thin hollow needles into the prostate. The needles fill with tissue which then goes to a laboratory for microscopic examination.
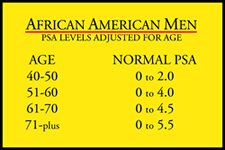
Biopsies are commonly ordered following an examination that combines a blood test to measure the level of prostate-specific antigen (PSA) in the blood, and a digital rectal examination (DRE). (insert A-A men table)
 |
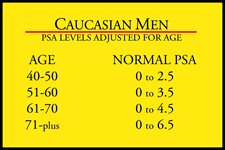 |
The nearby tables show how different levels of PSA indicate the possibility of prostate cancer. For example, Caucasian men between ages 51 and 60 have a very low risk of prostate cancer when their PSA level is below 3.5. A level above 3.5 increases the chance of cancer, and the higher the level above 3.5 the higher the risks. For example, cancer is present in one of every two men with a PSA higher than 10.0.
The combination of PSA and DRE can discover more than 75% of prostate cancers before they spread.
Any man old enough to be at risk of prostate cancer, and who fails to maintain the Society's "Assurance Policy against Death from Prostate Cancer" has only himself to blame if cancer is detected too late to cure.
The policy shown here in reduced size is available on request at no charge.
Illustration: "The Assurance Policy Against Death From Prostate Cancer." How it works: You post the results of each prostate exam including PSA and DRE by the month/year of the exams for up to 5 years. If (1) PSA climbs into "red flag" levels, or (2) the doctor's DRE finds something suspicious, you are virtually guaranteed your cancer will be caught while it is in its earliest stages and curable. Nobody dies from a cured cancer!
Curing Prostate Cancer
Never lose sight of the just-stated characteristic of prostate cancer: It can be cured.
That's great to know. But it also comes with a huge problem.
To be curable, the cancer must be found before it breaks through the prostate wall and spreads.
Five choices are available to each man when prostate cancer has been confirmed. In reviewing the choices, do NOT let anyone rush you into a decision. Prostate cancer grows so slowly it takes about four years for an average tumor to double in size. This means you have plenty of time to gain full knowledge of prostate cancer, and how your age, health, and love-life affect your alternatives.
URGENT! What follows is taken from our UPDATE newsletter "Prostate Cancer. When Should It Be Treated. And When Should It Be Left Alone?" Like everything from the Society, it is free on request. Other UPDATES cover additional aspects of prostate cancer, such as the status of research for a non-surgical/radiation cure.
Choice 1. Watch and wait. Deciding on this option involves the man's age, health, Gleason Score, and feelings about surgery and radiation.
Choice 2. External beam radiation. (EBRT) The desirability of this option depends on the sophistication of the available radiation equipment, the skill of the oncologist, and recognition that the effects of the treatment are irreversible.
Choice 3. Surgery. Generally considered the only sure cure. Generally ruled out for any man with less than 10 years of life expectancy. Major side effects. Success, including quality of life, varies enormously depending on the experience of the surgeon. More than half of all men who elect surgery become impotent.
Choice 4: Internal radiation with radioactive "seeds." Advantage is less side effects than other choices. Lacks long-term proof of effectiveness.
Choice 5: A combination of EBRT and radioactive seeding. Probably more effective than either radiation alone, but not yet an ideal selection.
For any of the four treatments to cure the cancer, as noted it must be confined to the prostate. Alas, there is no positive way to confirm that status. Therefore, to put it bluntly, a doctor who recommends surgery or any type of radiation as a cure of prostate cancer is making an educated guess.
His/her guess is based on a combination of the tumor's size and location(s), PSA and Gleason score.
The national average for educated guesses is 50% right, 50% wrong. A toss of a coin.
However, the very best hospitals, and the very best urologists, are much more successful in predicting the confined/not-confined status of the cancer. Urologists at Johns Hopkins, the University of Maryland, Mayo Clinic, and M.D. Anderson, to name a few, average 75% accuracy, or better. This means that some hospitals, and some less-skilled urologists are guessing right less than half the time.
How do you find a treatment center, or a doctor, you can trust with your life? There's just one way: ask tough questions.
This gets tricky. No one likes to seem to doubt the doctor you're about to entrust with your life. But your fate, your quality of life, and your treatment outcome hang in the balance. Not just for you, but for your family.
So screw up your nerve. One way or another get the answers you must have in reaching your decision. (If necessary, write out the questions and hand them to your doctor explaining you got them from The .)
Is your doctor/oncologist board certified? (If not, go elsewhere fast.)
How many prostates has he removed, or radiated, in the last six months? (The correct answer for surgeons is no less than one per month ---- and that's a minimum! )
Is he successful in sparing the nerve bundles necessary for penis erection? (If not, you will be impotent the rest of your life. External radiation does not spare these nerves.)
What percentage of his patients have regained satisfactory sexual activity? Does that percentage of satisfaction apply to you? Will you be satisfied with it for the rest of your life?
What percentage of his patients have become incontinent? What is his prediction for your continence - when will you regain continence after your treatments end?
If you doctor isn't so proud of his record he happily answers your questions, he has something to hide. Make sure that something isn't you.
One thing more! No matter how satisfied you are with your doctor, no matter how pleased you are with answers to your questions, whatever you do you MUST get at least ONE additional opinion.
Remember, your decision brings actions that can never be reversed. The results are forever. Whatever you decide, you must be able to say that your decision was based on weighing ALL knowledge available, plus the recommendation of more than one medical professional.
And another thing more! If you are married, the outcome of your decision will affect your wife as well as you. Remember that half or more of prostate operations result in impotent men. Be guided accordingly. Survivors of prostate cancer agree 100% that sharing your fears, doubts, hopes and other feelings with those who love you will make everyone feel better no matter the actual outcome of your decision.
TREATMENTS THAT FAIL
This is a complex subject involving life and death itself. Due to the sensitivity of failed cancer treatments, and the need for clear understanding of every implication, interested persons should request our UPDATE newsletter on cures that fail, and PC-SPES. All survivors of prostate cancer treatments should join the Society to keep abreast of any new developments affecting treatments that have failed.